Ob Gyn History Template - Have you ever had (please mark with estimated date): Of type of complications mother. Do you have a history of pcos (polycystic ovary syndrome)? Use this free ob gyn patient history form template to collect information from patients about past pregnancies, medical conditions, and current. Review of systems (check all that apply and explain if necessary) Do you have a history. Place of delivery duration hrs. Have you had a cervical biopsy? Please list any past surgeries and dates: History of abnormal pap smear?
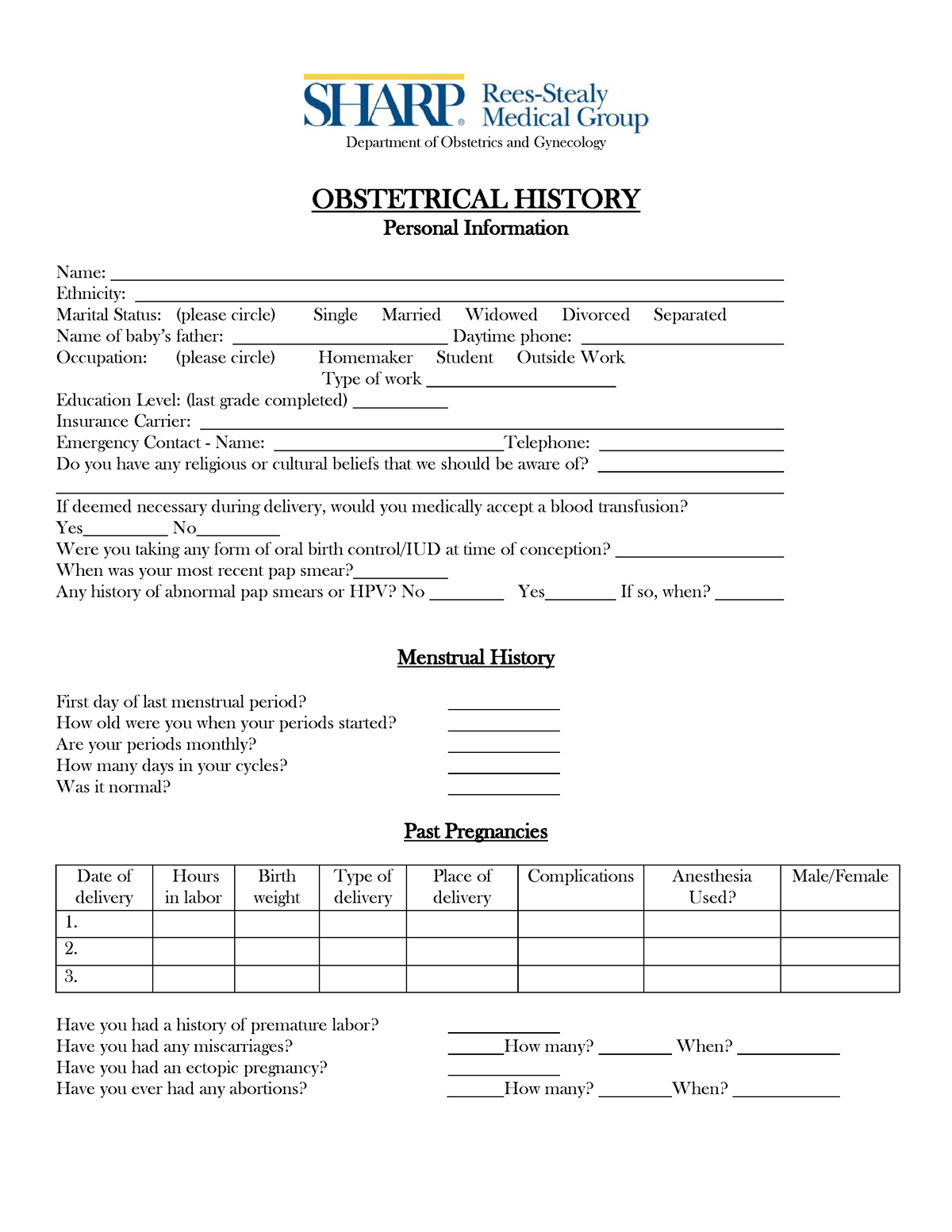
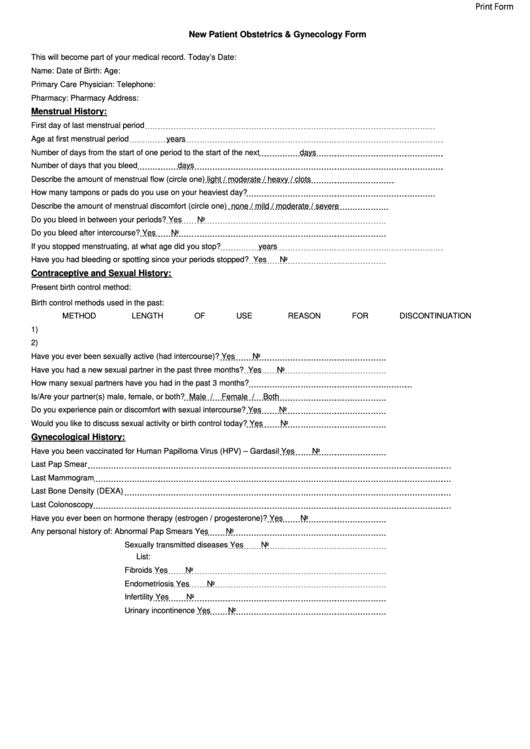
Use this free ob gyn patient history form template to collect information from patients about past pregnancies, medical conditions, and current. Obstetrical history including abortions & ectopic (tubal) pregnancies. History of abnormal pap smear? Have you had a cervical biopsy? Do you have a history of pcos (polycystic ovary syndrome)? Of type of complications mother. Have you had any bleeding since your last period? Have you ever had (please mark with estimated date): What was the first day of your last normal period? Review of systems (check all that apply and explain if necessary)
Do you have a history of pcos (polycystic ovary syndrome)? Review of systems (check all that apply and explain if necessary) Have you ever had (please mark with estimated date): Obstetrical history including abortions & ectopic (tubal) pregnancies. Use this free ob gyn patient history form template to collect information from patients about past pregnancies, medical conditions, and current. Do you normally have a period every month? Place of delivery duration hrs. Please list any past surgeries and dates: Have you had any bleeding since your last period? Of type of complications mother.

Established Patient Prenatal Medical History Form Santa Fe Ob/Gyn
Do you normally have a period every month? History of abnormal pap smear? Do you have a history. Obstetrical history including abortions & ectopic (tubal) pregnancies. What was the first day of your last normal period?
Ob Gyn History Template
Please list any past surgeries and dates: Do you have a history. Review of systems (check all that apply and explain if necessary) Have you had any bleeding since your last period? Do you normally have a period every month?

OBGYN Patient History Form Template OnTask
Review of systems (check all that apply and explain if necessary) Do you have a history. Have you had any bleeding since your last period? Do you have a history of pcos (polycystic ovary syndrome)? Place of delivery duration hrs.

WriteUp Sample Obstetrics and Gynecology History Taking PDF
Have you had any bleeding since your last period? Have you had a cervical biopsy? History of abnormal pap smear? Of type of complications mother. Do you normally have a period every month?
Obgyn History Template
Have you ever had (please mark with estimated date): History of abnormal pap smear? Do you have a history. Please list any past surgeries and dates: Place of delivery duration hrs.
Printable Ob History Form Printable Forms Free Online
Have you had any bleeding since your last period? What was the first day of your last normal period? Do you normally have a period every month? Do you have a history. Review of systems (check all that apply and explain if necessary)
OBGYN Intake Form Digital Download Obstetrical History Form Printable
Do you have a history. Do you have a history of pcos (polycystic ovary syndrome)? Have you ever had (please mark with estimated date): What was the first day of your last normal period? Have you had any bleeding since your last period?
OB HX form Obstetric History Form sample format Department of
Have you had any bleeding since your last period? Do you normally have a period every month? Do you have a history of pcos (polycystic ovary syndrome)? Review of systems (check all that apply and explain if necessary) Place of delivery duration hrs.
Obgyn History Template
Obstetrical history including abortions & ectopic (tubal) pregnancies. Have you ever had (please mark with estimated date): What was the first day of your last normal period? Do you have a history of pcos (polycystic ovary syndrome)? Please list any past surgeries and dates:

History Taking Form in Gynecology & Obstetrics Vomiting Nausea
Place of delivery duration hrs. Have you had a cervical biopsy? Have you had any bleeding since your last period? Do you have a history of pcos (polycystic ovary syndrome)? Do you normally have a period every month?
Have You Had Any Bleeding Since Your Last Period?
Use this free ob gyn patient history form template to collect information from patients about past pregnancies, medical conditions, and current. Place of delivery duration hrs. Do you have a history. Do you normally have a period every month?
Please List Any Past Surgeries And Dates:
Obstetrical history including abortions & ectopic (tubal) pregnancies. Review of systems (check all that apply and explain if necessary) Have you ever had (please mark with estimated date): Do you have a history of pcos (polycystic ovary syndrome)?
Of Type Of Complications Mother.
What was the first day of your last normal period? Have you had a cervical biopsy? History of abnormal pap smear?