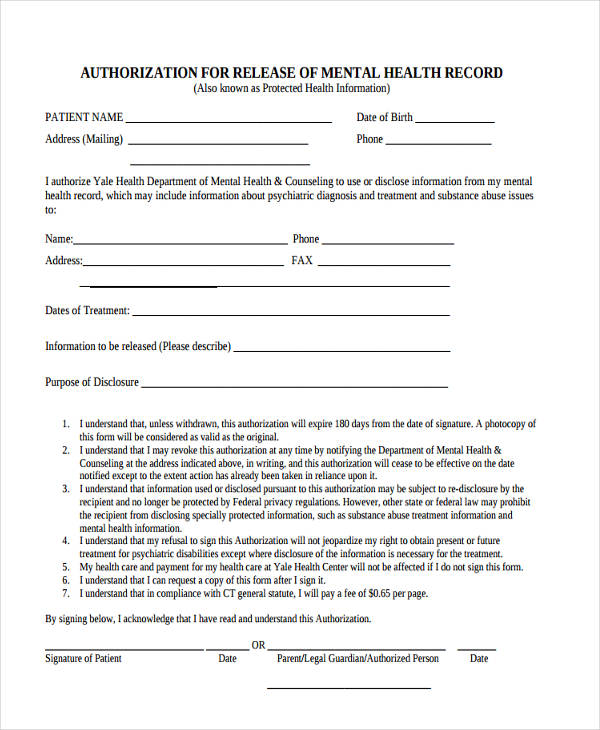
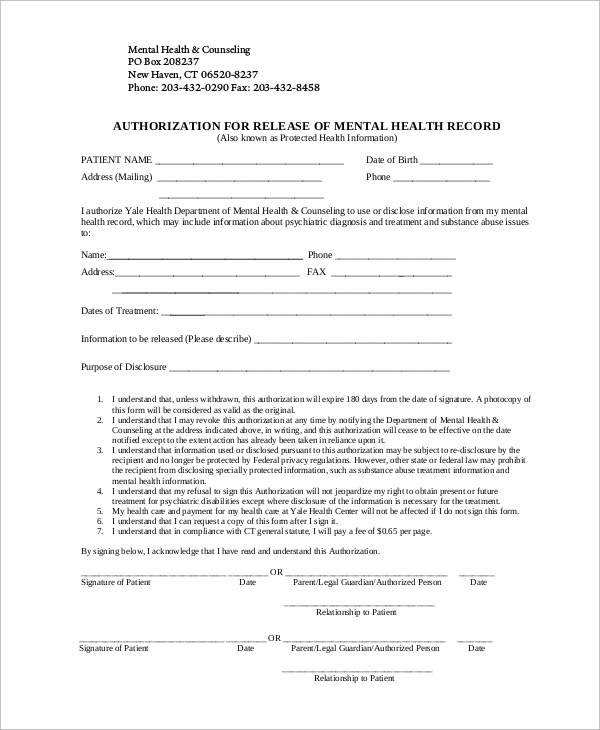
Release Of Information Form Template Mental Health - That my signing of this authorization is voluntary. By signing this form, confidential psychological and psychiatric information can be released to and/or discussed with the people or agencies listed. And/or hipaa 45 cfr) and state. I understand that any cancellation or modification of this authorization must be in. I am giving my permission to compass health to disclose my confidential health records. By signing below, i authorize the release. I understand that i have a right to receive a copy of this authorization. This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private. My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; Of my information as specified above.
I am giving my permission to compass health to disclose my confidential health records. By signing this form, confidential psychological and psychiatric information can be released to and/or discussed with the people or agencies listed. By signing below, i authorize the release. I understand that i have a right to receive a copy of this authorization. This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private. That my signing of this authorization is voluntary. Of my information as specified above. I understand that any cancellation or modification of this authorization must be in. And/or hipaa 45 cfr) and state. My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2;
I am giving my permission to compass health to disclose my confidential health records. That my signing of this authorization is voluntary. And/or hipaa 45 cfr) and state. By signing this form, confidential psychological and psychiatric information can be released to and/or discussed with the people or agencies listed. Of my information as specified above. By signing below, i authorize the release. I understand that i have a right to receive a copy of this authorization. My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; I understand that any cancellation or modification of this authorization must be in. This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private.
FREE 22+ Release of Information Form Samples, PDF, MS Word, Google Docs
By signing below, i authorize the release. My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; I understand that i have a right to receive a copy of this authorization. I understand that any cancellation or modification of this authorization must be in. And/or hipaa 45 cfr) and state.
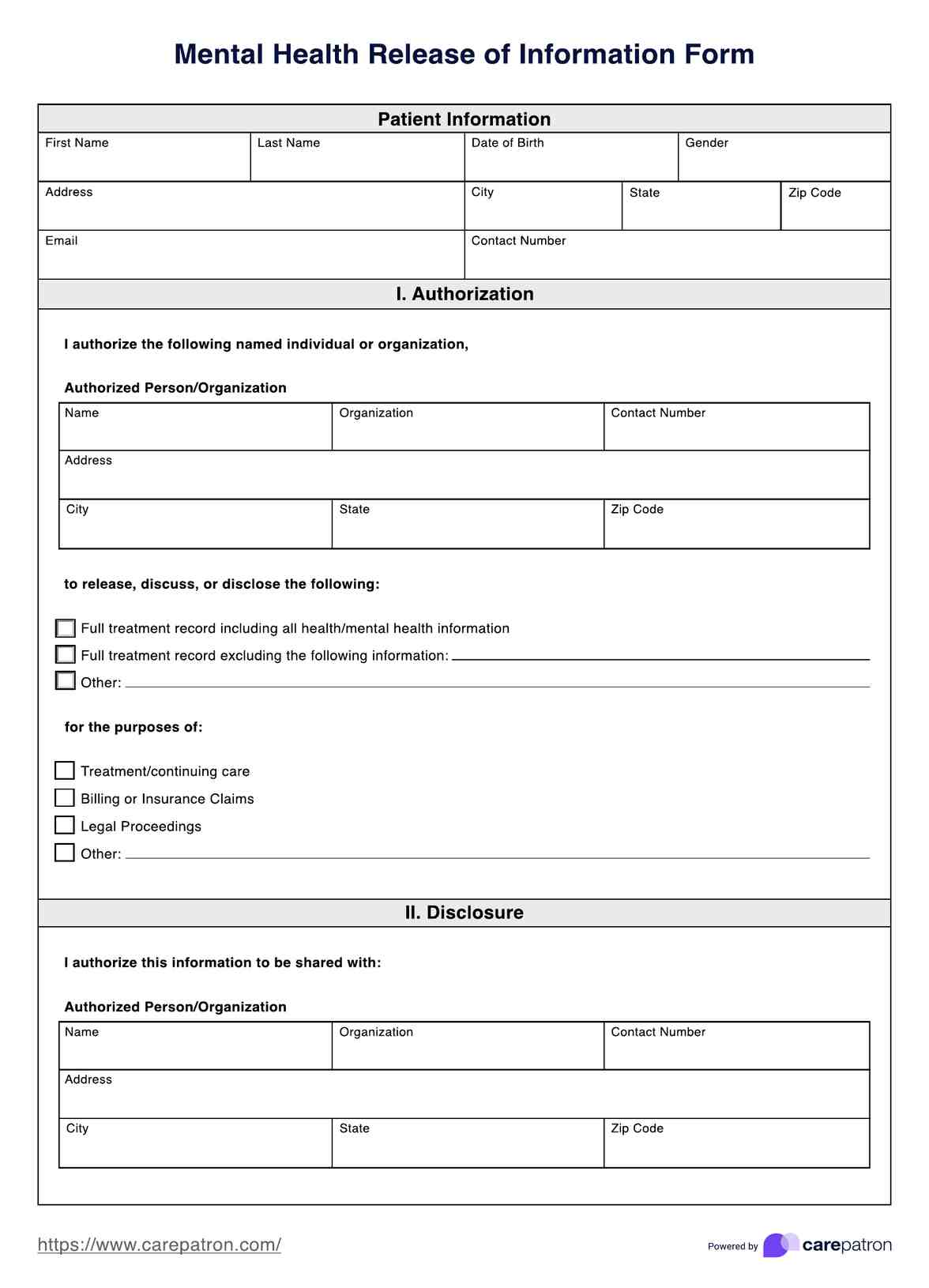
Printable Mental Health Release Form
And/or hipaa 45 cfr) and state. By signing below, i authorize the release. I understand that any cancellation or modification of this authorization must be in. By signing this form, confidential psychological and psychiatric information can be released to and/or discussed with the people or agencies listed. I understand that i have a right to receive a copy of this.

Release Of Information Form Template Mental Health
I understand that any cancellation or modification of this authorization must be in. By signing this form, confidential psychological and psychiatric information can be released to and/or discussed with the people or agencies listed. Of my information as specified above. By signing below, i authorize the release. My health information is protected by federal regulation (alcohol & drug abuse patient.
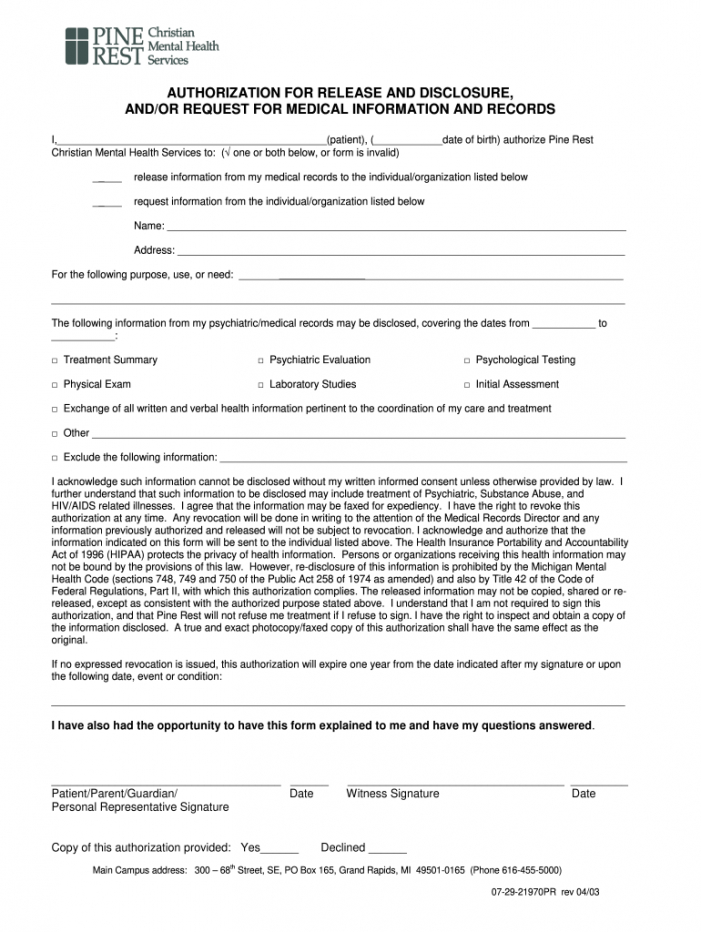
Release Of Information Form Template Mental Health
And/or hipaa 45 cfr) and state. I am giving my permission to compass health to disclose my confidential health records. That my signing of this authorization is voluntary. By signing below, i authorize the release. This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private.

Release Of Information Form Template Mental Health
This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private. And/or hipaa 45 cfr) and state. Of my information as specified above. I understand that any cancellation or modification of this authorization must be in. By signing this form, confidential psychological and psychiatric information can be released.
Mental Health Release Of Information Form & Template Free PDF Download
This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private. By signing this form, confidential psychological and psychiatric information can be released to and/or discussed with the people or agencies listed. By signing below, i authorize the release. I understand that any cancellation or modification of this.
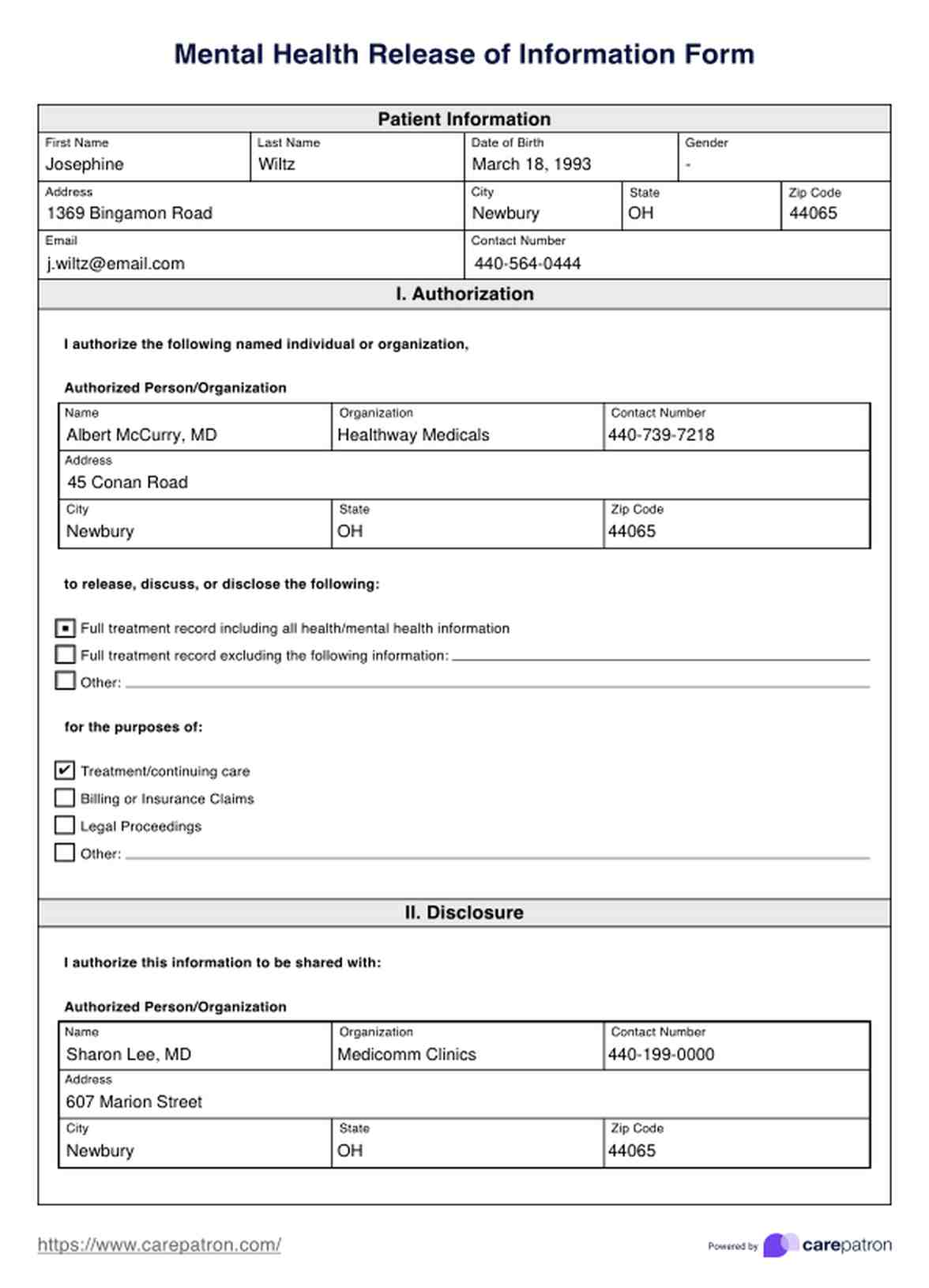
Mental Health Release of Information Form & Template Free PDF Download
My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; I understand that any cancellation or modification of this authorization must be in. By signing this form, confidential psychological and psychiatric information can be released to and/or discussed with the people or agencies listed. By signing below, i authorize the release. I.

Mental Health Release Of Information Template
By signing this form, confidential psychological and psychiatric information can be released to and/or discussed with the people or agencies listed. This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private. I understand that any cancellation or modification of this authorization must be in. Of my information.

Mental Health Release Of Information Form & Template Free PDF Download
I understand that i have a right to receive a copy of this authorization. And/or hipaa 45 cfr) and state. I am giving my permission to compass health to disclose my confidential health records. This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private. My health information.
FREE 9+ Sample Release of Information Forms in MS Word PDF
That my signing of this authorization is voluntary. This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private. By signing this form, confidential psychological and psychiatric information can be released to and/or discussed with the people or agencies listed. I am giving my permission to compass health.
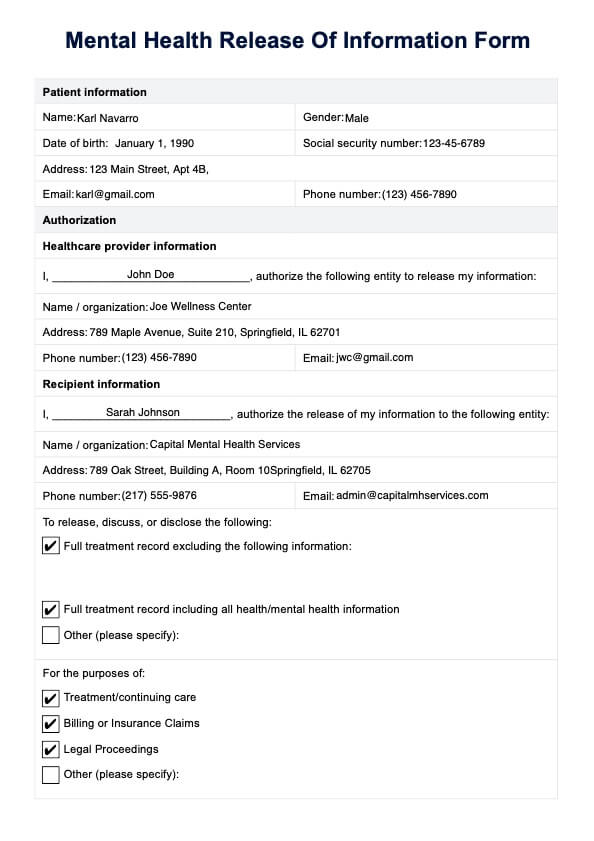
By Signing This Form, Confidential Psychological And Psychiatric Information Can Be Released To And/Or Discussed With The People Or Agencies Listed.
I understand that any cancellation or modification of this authorization must be in. My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; I am giving my permission to compass health to disclose my confidential health records. And/or hipaa 45 cfr) and state.
I Understand That I Have A Right To Receive A Copy Of This Authorization.
This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private. By signing below, i authorize the release. That my signing of this authorization is voluntary. Of my information as specified above.